


Cushing's Syndrome
On this page:
- What is Cushing’s syndrome?
- How common is Cushing’s syndrome?
- Who is more likely to have Cushing’s syndrome?
- What are the complications of Cushing’s syndrome?
- What are the symptoms of Cushing’s syndrome?
- What causes Cushing’s syndrome?
- How do doctors diagnose Cushing’s syndrome?
- How do doctors find the cause of Cushing’s syndrome?
- How do doctors treat Cushing’s syndrome?
- Clinical Trials
What is Cushing’s syndrome?
Cushing’s syndrome is a disorder that occurs when your body makes too much of the hormone cortisol over a long period of time. Cortisol is sometimes called the “stress hormone” because it helps your body respond to stress. Cortisol also helps
- maintain blood pressure
- regulate blood glucose, also called blood sugar
- reduce inflammation
- turn the food you eat into energy
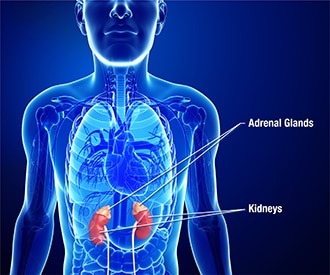
The adrenal glands, two small glands on top of your kidneys, make cortisol.
How common is Cushing’s syndrome?
Endogenous Cushing’s syndrome is rare. “Endogenous” means something inside your body is causing the disorder rather than something outside your body, such as medicine. Estimates vary, ranging from about 40 to 70 people out of every million.1
Who is more likely to have Cushing’s syndrome?
Cushing’s syndrome most often affects adults, usually aged 30 to 50,1 but can also occur in children. Cushing’s syndrome affects about three times as many women as men.2 In people who have type 2 diabetes and blood glucose levels that stay too high over time, along with high blood pressure, Cushing’s syndrome may be the cause. People who take medicines called glucocorticoids, which are similar to cortisol, also can develop Cushing’s syndrome. This type of Cushing’s syndrome is called “exogenous.” More than 10 million Americans take glucocorticoids each year,3 but it’s not known how many of them develop Cushing’s syndrome.
What are the complications of Cushing’s syndrome?
Cushing’s syndrome can cause health problems such as
- heart attack and stroke
- blood clots in the legs and lungs
- infections
- bone loss and fractures
- high blood pressure
- unhealthy cholesterol levels
- depression or other mood changes
- memory loss or trouble concentrating
- insulin resistance and prediabetes
- type 2 diabetes
Although Cushing’s syndrome can usually be cured, it can be fatal if not treated.
What are the symptoms of Cushing’s syndrome?
Signs and symptoms of Cushing's syndrome vary. People who have very high levels of cortisol for a long time are likely to have clear signs of the disorder, including
- weight gain
- thin arms and legs
- a round face
- increased fat around the base of the neck
- a fatty hump between the shoulders
- easy bruising
- wide purple stretch marks, mainly on the abdomen, breasts, hips, and under the arms
- weak muscles
Children with Cushing’s syndrome tend to have obesity and grow more slowly than other children. Women may have excess hair on their face, neck, chest, abdomen, and thighs. Menstrual periods may become irregular or stop. Men may have decreased fertility with lowered interest in sex and may have erectile dysfunction.
Not everyone with Cushing’s syndrome has these symptoms, which can make it hard to detect.
What causes Cushing’s syndrome?
The most common cause of Cushing’s syndrome is the long-term, high-dose use of the cortisol-like glucocorticoids. These medicines are used to treat other medical conditions, such as asthma, rheumatoid arthritis, and lupus. Glucocorticoids are often injected into a joint to treat pain. Use of glucocorticoids also suppresses the immune system after an organ transplant to keep the body from rejecting the new organ.
Other people develop endogenous Cushing’s syndrome because their bodies make too much cortisol. Several types of tumors can cause the body to make excess cortisol.
Pituitary tumors
Pituitary tumors, also called pituitary adenomas, are noncancerous growths on the pituitary gland. The pituitary gland sits at the base of the brain and is about the size of a pea. The pituitary makes adrenocorticotropic hormone (ACTH) and other hormones. ACTH tells the adrenal glands to make cortisol. These pituitary tumors make too much ACTH, causing the adrenals to make too much cortisol.

Pituitary tumors that make too much ACTH cause 8 out of 10 cases of Cushing’s syndrome2 not caused by glucocorticoid medicines. Doctors call this type of Cushing’s syndrome Cushing’s disease.
Ectopic ACTH-producing tumors
Some tumors that develop outside the pituitary gland also can produce ACTH. This condition is called ectopic ACTH syndrome. Most often, these tumors occur in the lungs. Ectopic tumors also can occur in the pancreas, thyroid, and thymus—a gland that helps build a healthy immune system. Ectopic tumors may be cancerous.
Adrenal tumors
Sometimes a tumor on the adrenal gland itself makes too much cortisol. Adrenal tumors are most often benign but sometimes are cancerous.
How do doctors diagnose Cushing’s syndrome?
Cushing’s syndrome can be hard to diagnose. Symptoms such as fatigue and weight gain can have many different causes. Cushing’s syndrome may be mistaken for other conditions that have many of the same signs, such as polycystic ovary syndrome or metabolic syndrome. Your doctor will first want to rule out other conditions.
Diagnosis is based on your medical history, a physical exam, and lab tests. Your doctor may ask if you are taking glucocorticoids or have had injections and rule that out before ordering lab tests.
Doctors may use urine, saliva, or blood tests to diagnose Cushing’s syndrome. Sometimes doctors run a follow-up test to find out if excess cortisol is caused by Cushing’s syndrome or has a different cause.
No one test is perfect, so doctors usually do two of the following tests to confirm a diagnosis:
24-hour urinary free-cortisol test
In this test, you will collect your urine over a 24-hour period. Your health care professional will send your urine sample to a lab to test cortisol levels. Higher than normal cortisol levels suggest Cushing’s syndrome.
Late-night salivary cortisol test
This test measures the amount of cortisol in your saliva in the late evening. Normally, cortisol production drops just after we fall asleep. In Cushing’s syndrome, cortisol levels don’t drop. You can collect your saliva sample at home and return it to your health care professional or send it to a lab for testing.
Low-dose dexamethasone suppression test (LDDST)
In this test, you will take a low dose of dexamethasone, a type of glucocorticoid, usually around 11:00 p.m. A health care professional will draw your blood the following morning, usually around 8 a.m. Sometimes doctors use another type of LDDST test, in which you take dexamethasone every 6 hours for 48 hours. Your blood is drawn 6 hours after the last dose.
Normally, cortisol levels in the blood drop after taking dexamethasone. Cortisol levels that don’t drop suggest Cushing’s syndrome.

When one of the first blood tests show that your body has too much cortisol, your doctor may order a follow-up test, called the dexamethasone–corticotropin-releasing hormone (dexamethasone-CRH) test.
Dexamethasone–CRH test
The dexamethasone-CRH test shows whether excess cortisol is caused by Cushing’s syndrome or by something else.
Some people have high cortisol levels off and on but don’t develop the long-term health effects of Cushing's syndrome. These people may have pseudo-Cushing's syndrome, a condition sometimes found in people who have depression or anxiety, drink too much alcohol, have diabetes with blood glucose levels that are often too high, or have obesity.
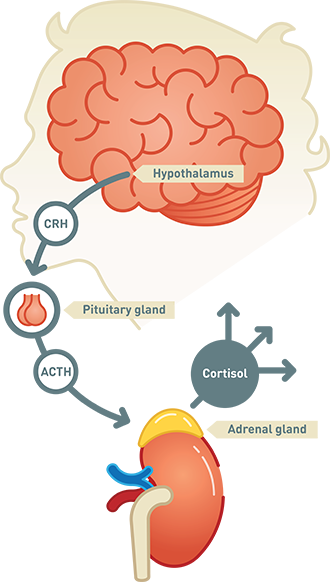
This test combines the LDDST and a CRH stimulation test. CRH is a hormone made in the part of the brain called the hypothalamus. CRH tells the pituitary to make ACTH, which in turn tells the adrenals to make cortisol. When cortisol levels rise enough, they turn off the CRH signal, so ACTH and cortisol levels fall.
You’ll get a shot of CRH and take dexamethasone by mouth. If you have pseudo-Cushing’s syndrome, the dexamethasone will decrease ACTH and cortisol levels and keep them from rising. Cortisol levels that are high just before the CRH shot or rise during this test suggest Cushing's syndrome.
How do doctors find the cause of Cushing’s syndrome?
Once your doctor diagnoses Cushing’s syndrome, other tests can help tell whether the source of the problem is pituitary, ectopic, or adrenal. Knowing the source is important in choosing the best type of treatment.
Blood tests
The first step is to measure ACTH levels in the blood. If ACTH levels are low, the cause is probably an adrenal tumor. People with adrenal tumors don’t need further blood tests.
If ACTH levels are normal or high, the cause is probably a pituitary or ectopic tumor.
Other blood tests help tell pituitary tumors from ectopic tumors. Doctors usually do more than one test.
CRH stimulation test. For this test, you’ll get a shot of CRH. If you have a pituitary tumor, CRH will increase the ACTH and cortisol in your blood. This rarely happens in people with ectopic tumors.
High-dose dexamethasone suppression test (HDDST). This test is the same as the LDDST, except it uses higher doses of dexamethasone. If the cortisol levels in your blood drop after taking a high dose of dexamethasone, you probably have a pituitary tumor. If your cortisol levels don’t drop, you may have an ectopic tumor.
Other tests
Other tests look for tumors and help tell pituitary tumors from ectopic tumors.
Imaging tests. Imaging tests show the size and shape of the pituitary and adrenal glands and look for tumors. If blood tests show that the tumor is ectopic, imaging tests can help locate the tumor. The most common imaging tests are the computerized tomography (CT) scan and magnetic resonance imaging (MRI).

Petrosal sinus sampling. Pituitary tumors are usually small and may not show up in an imaging test. If an MRI doesn’t show a pituitary tumor, you might have petrosal sinus sampling. This test is often the best way to tell pituitary from ectopic causes of Cushing's syndrome.
Your doctor will draw samples of blood from your petrosal sinuses—veins that drain the pituitary. At the same time, you will have a blood sample taken from a blood vessel far away from the pituitary. You will also get a shot of CRH, the hormone that causes the pituitary to release ACTH.
Higher levels of ACTH in the blood from the petrosal sinuses than from the other blood vessel indicate a pituitary tumor. Similar levels of ACTH in all the blood samples suggest an ectopic tumor.
How do doctors treat Cushing’s syndrome?
Treatment depends on the cause and may include surgery, radiation, chemotherapy, or cortisol-reducing medicines. If the cause is long-term use of glucocorticoids to treat another disorder, your doctor will gradually reduce your dosage to the lowest dose that will control that disorder. Sometimes disorders that doctors treat with glucocorticoids can be treated with a non-glucocorticoid medicine instead.
Pituitary tumors
The most common treatment for pituitary tumors is surgery to remove the tumor. Using a special microscope and fine instruments, a surgeon approaches the pituitary gland through a nostril or an opening made below the upper lip. Your doctor will probably refer you to a center specializing in this type of surgery.
The success, or cure, rate of this surgery can be as high as 90 percent when done by a highly experienced surgeon.4 If surgery fails or the cure doesn’t last, surgery can be repeated, often with good results.

After the surgeon removes the tumor, your pituitary won’t make enough ACTH for a while. Your doctor will prescribe cortisol medicine since there’s not enough ACTH to tell the adrenal glands to make enough cortisol. You may be able to stop cortisol medicine in 6 to 18 months.
If surgery fails or isn’t possible, radiation therapy is an option. One type of radiation therapy uses small doses of radiation to the pituitary over a 6-week period. Another type uses a single, high dose of radiation. Cortisol levels may not return to normal after radiation therapy for several years. Your doctor may prescribe medicines to bring cortisol levels back to normal until radiation therapy takes effect.
Ectopic ACTH-producing tumors
The first choice of treatment for ectopic tumors is to remove them surgically. If the tumor is cancerous and has spread, you may need chemotherapy, radiation therapy, or other cancer treatments. Medicines to reduce cortisol levels may also be part of your treatment. If other treatments fail, surgeons might have to remove the adrenal glands to control Cushing’s syndrome.
Adrenal tumors
Surgery to remove the adrenal gland with the tumor is the most common treatment. Some rare diseases cause many nodules in both adrenal glands and require surgery to remove both glands. If you have both adrenal glands removed, you will need to take medicine for life to replace cortisol and other hormones the adrenal glands make.
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you.
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at ClinicalTrials.gov.
References
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases
(NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.